
Spring 2024 distributed quarterly to 2900 optometric physicians
From the EDITOR As optometric physicians, anterior uveitis is one of the most common causes of ocular inflammation that we encounter. We are usually the first practitioners to see and treat this disease, so it is important for us to manage these patients appropriately and effectively. In this issue, my colleague Brett Igbinoba reviews the acute type of anterior uveitis, which is also the most prevalent.

Back to basics
By Brett Igbinoba, OD | PCLI—BELLINGHAM, WA
Anterior Uveitis

Ami Halvorson, OD
PCLI—Portland, OR
We’ve likely all been in this situation. A patient calls the office pleading to be seen, claiming an inordinate amount of pain in one eye. After working them into your schedule, they arrive 20 minutes early wearing oversized dark sunglasses in the waiting room. They can’t fathom opening their eye for the technician’s tests. When you enter the exam room, all light sources are off. You examine the anterior chamber using the smallest, faintest parallelepiped possible and discover little white cells merrily floating about.
Now what?
Acute Anterior Uveitis
Uveitis is, of course, inflammation of the uveal tract. But for this discussion, let’s focus on diagnosing and managing the most prevalent type—acute anterior uveitis (AAU).
Uveitidies account for up to 20% of blindness in the United States. This inflammatory disease can either be an isolated condition or a sign of systemic inflammation. Although AAU is the most common type of uveitis and contributes the least to potential blindness, its sequelae can be visually compromising. So, we must treat it swiftly and with confidence.
AAU is defined as the sudden onset of inflammation in the front of the eye involving the iris and/or ciliary body. Other terms, such as iritis, cyclitis, and iridocyclitis, are often used interchangeably because clinically differentiating inflammation of the iris and ciliary body can be challenging.
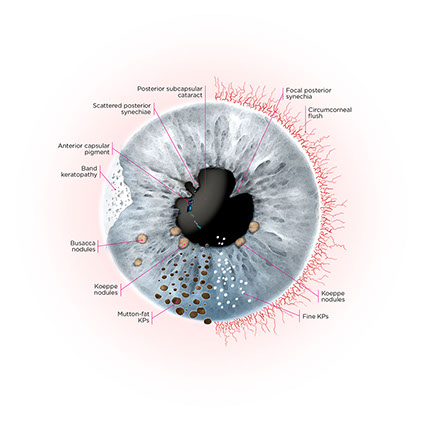
Clinical Signs of
Anterior Uveitis
Causes
The most common etiology is idiopathic. AAU is also likely in cases of trauma or intraocular surgery. Most systemic associations correlate with the genotype Human Leukocyte Antigen—B27 (HLA B27). Rarer systemic associations are also inflammatory in nature, and a non-exhaustive list includes herpes simplex/zoster/CMV, interstitial nephritis, multiple sclerosis, syphilis, and Lyme disease.
Diagnosis
AAU can be diagnosed based on the patient’s symptoms and clinical appearance. Usual complaints include:
- Dull pain
- Photophobia
- Conjunctival injection
- Excessive tearing
- Varying degrees of visual blur
The clinical exam will reveal either circumlimbal or diffuse conjunctival injection, fine keratic precipitates on the endothelium, and pathognomonically cells (and possibly flare) in the anterior chamber. Other findings typically include fibrinous exudate, iris nodules and atrophy, posterior synechiae, heterochromia iridis, iris neovascularization, and anomalous (elevated or lowered) intraocular pressure.
Grading
Proper grading of the AC reaction is essential in determining initial treatment dosing, its efficacy, and taper schedule. In 2005, the Standardization of Uveitis Nomenclature (SUN) working group, made up of uveitis specialists from around the world, developed standard grading scales that enable all providers to be on the same page when treating patients.
SUN Grading for AC Cells
Grade
Cells in field
0
0.5+
1+
2+
3+
4+
< 1
1 - 5
6 - 15
16 - 25
26 - 50
50+
(using 1mm x 1mm slit beam)
SUN Grading for AC Flare
FLARE
Description
0
1+
2+
3+
4+
None
Faint – faint haze in AC, iris and lens clearly visible
Moderate – iris and lens details clear
Marked – iris and lens details hazy
Intense – fibrin or plastic-appearing aqueous
Treatment
Treatment consists of controlling inflammation and managing the patient’s pain. Corticosteroids are the mainstay, and the key is being aggressive. Treatment of moderate to severe cases should be with a potent steroid, such as prednisolone acetate 1%, dosed 1 drop every hour while awake, or difluprednate 0.05%, dosed 1 drop every 2 hours while awake. Less-potent steroids, such as loteprednol, fluoromethalone, or prednisolone acetate 0.5% are possible. However, these medications’ reduced availability and premium costs should be considered.
The steroid should not be tapered until the AC reaction has decreased. For example, a patient presenting with 2+ cells might be treated with PA 1% at Q1h. If the AC shows 0.5+ to 1+ cells a few days later, it would be appropriate to taper the dose to Q2h until their next follow-up visit. However, I prefer not to begin tapering until the cell grade is 0.5+ or 0.
Cycloplegic agents are greatly beneficial in the management of AAU. They improve patient discomfort by paralyzing the iris sphincter and ciliary muscle. This action also prevents and helps break posterior synechiae by dilating the eye and keeping the pupil mobile. Cycloplegics also reduce flare by stabilizing the blood-aqueous barrier. Cyclopentolate is an effective and widely available cycloplegic agent. Homatropine and scopolamine are also helpful in cycloplegia, but regional availability can vary.
Tips for
Cataract Surgery
Follow-up Care
Follow-up depends on the severity of the initial inflammation. When patients present with mild symptoms, weekly follow-up is appropriate. Patients with 2 to 3+ AC cells who are highly symptomatic should be seen within a day or two to ensure they improve. Then, every three to seven days is appropriate. When herpes is on your list of differentials, seeing patients within three days of initiating treatment is beneficial. If an oral antiviral was not initially prescribed, the steroid may induce a corneal lesion. Closer follow-up will allow treatment to be adjusted accordingly.
If patients do not improve with treatment, lab tests should be ordered.
Lab Tests
Uveitis laboratory tests can seem daunting. While they are not necessary for first documented cases, testing is required if the uveitis is severe, bilateral, granulomatous, or is a recurrence. Although the following is not an all-inclusive list of lab tests, they are more commonly ordered to differentiate based on the patient’s symptom and systemic profile: RPR, VDRL, FTA-ABS, PPD, chest x-ray, ACE, Lyme titer, ESR, RF, and/or HLA-B27.
Conclusion
Primary care optometrists can effectively manage and care for AAU with steroid and cycloplegic eyedrops. The key is to treat it aggressively and not taper drops too quickly. This typically results in a straightforward healing process for which patients are grateful.
Questions If you have questions, feel free to contact any of our optometric physicians. We’re always happy to help.
ABOUT THE AUTHOR
Brett Igbinoba
PCLI BELLINGHAM, WA
Positive, compassionate and reassuring, Brett Igbinoba enjoys listening, finding solutions, and letting people know that no concern is too big or too small to talk about and treat. Born in Spokane, Washington, Brett grew up nearby in Cheney. He enjoys exercising, snowboarding, camping and traveling. He and his wife, Jen, a strength and conditioning coach, live in Bellingham, Washington. They have a daughter and a son—Maya and Quincy.

Share