
SUMMER 2024 distributed quarterly to 2900 optometric physicians
From the EDITOR The iris is arguably one of the eye’s most intricately delicate and beautiful tissues. When damaged, it can leave patients with uncomfortable functional and cosmetic symptoms. In this issue, my colleague and optometry school classmate, Brian Arvidson, reviews various iris anomalies and several management options.

AN OVERVIEW
By Brian Arvidson, OD | PCLI—CHEHALIS, WA
Iris Anomalies–

Ami Halvorson, OD
PCLI—Portland, OR
Iris anomalies, though rare, can significantly impact our patients’ vision and lifestyle. However, thanks to the ingenuity of skilled surgeons and device manufacturers, innovative techniques and technologies have been developed to address some of these challenges. Join me for a brief review of iris anomalies and several creative solutions.
Two Types
There are two types of iris anomalies: congenital and acquired. Each has a wide range of symptoms, including glare and halos, photophobia, and reduced vision.
- Congenital – Usually associated with poorer outcomes and significantly reduced visual potential.
- Acquired – Can affect the whole range of visual potential depending on the cause.
Let’s take a closer look at each.
CONGENITAL ANOMALIES
Congenital anomalies are rare, with several cases per 100,000 births, and vary in cause and presentation.
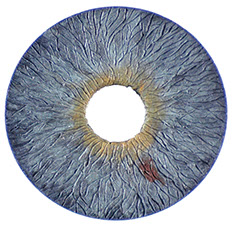
Aniridia – Partial or complete absence of the iris, which can be congenital or acquired. It is most commonly autosomal dominant (~85%), and its presentation may be sporadic secondary to de novo point mutations. Visual potential is usually poor secondary to concomitant conditions, most commonly strabismus and/or nystagmus.
Coloboma – A gap or notch in the iris that can vary in size and shape and is usually associated with reduced vision. They are due to incomplete development of the iris during gestation and rarely are the only presenting feature. Treatment is often amblyogenic therapy.
Ocular and oculocutaneous albinism – Stems from a deficiency of melanosomes in the iris. This uncommon disorder is inherited through X-linked or autosomal recessive patterns. The eye exhibits a pink hue due to light transmission through the iris, with visual impairment from associated conditions such as nystagmus, strabismus, high myopia, and retinal issues.
ACQUIRED IRIS ANOMALIES
Acquired iris anomalies can result from trauma (accidental or surgical), infection, and disease.
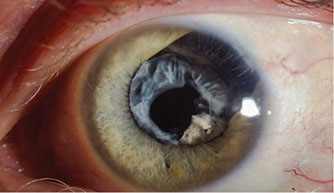
Trauma – The primary causes are blunt force, either with closed or open globe injury, penetrating wounds, or injuries caused by surgery. Anomalies may present as tears, breaks, thinning, or atrophy of the iris, leading to a wide array of symptoms.
Infections – Anomalies may arise from HSK or HSV. These herpetic infections can precipitate acute anterior uveitis and secondary synechiae or induce sectoral iris atrophy. The subsequent thinning of iris pigmentation elicits transillumination defects, which can trigger photophobia and dysphotopsia.
Disease – Iris defects can develop due to progressive disease or complications from unmanaged systemic conditions. Iridocorneal Endothelial Syndrome (ICE) results in varying degrees of corectopia through iris degeneration and displacement of the pupil. Additionally, as the atrophy progresses, polycoria can occur due to ischemic injury to the iris. These types of anomalies are associated with secondary angle closure glaucoma and corneal edema. Retinal complications and ischemic events may prompt angiogenesis or neovascularization in the iris and angle, potentially resulting in mechanical and/or ischemic pupillary abnormalities.
Treatment Options
So, what can be done? Several options may be available, depending on the case’s complexity, the amount of iris involved, and the potential for visual recovery.
NON-SURGICAL
Treatment may involve soft contact lenses with an artificial iris, an opaque ring-shaped design with a clear central pupil that can be customized for each patient’s needs. In cases of symptomatic focal iris sphincter atrophy or mydriasis, pharmaceutical therapy with cholinergic agonists can stimulate miosis.
SURGICAL
Depending on the extent of the iris pathology, surgical options include pupilloplasty, iris suturing of focal defects or iris cerclage, synthetic iris prosthesis, and pinhole IOLs.
Pupilloplasty – Focal tears and defects can be closed with an interrupted suture approximating the edges of the defect, reducing iris gaping and limiting aberrant light transmission.

Congenital aniridia
After surgery
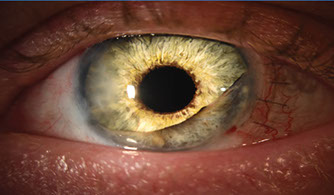
Iris cerclage – For patients suffering from mydriasis, without tears of the iris sphincter or root, a running suture can be used to encircle the pupillary ruff in a purse-string fashion.

Mydriasis
After surgery
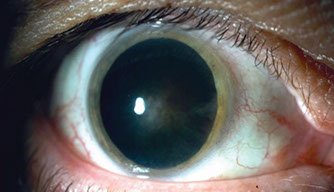
Artificial iris – The CUSTOMFLEX prosthetic is an FDA-approved device that can correct both cosmetic and subjective symptoms associated with iris anomalies. It can be sutured into place or positioned in the capsular bag or ciliary sulcus. The prosthetic can also be custom colored to match the fellow eye. Watch an interesting surgery video.
Click to View
CUSTOMFLEX implant

With prosthetic
Iatrogenic trauma
FLARE
Description

Congenital aniridia
With prosthetics

Piggyback pinhole implant – In Europe and several other countries, pseudophakic patients with irregular astigmatism or iris anomalies can benefit from the German-made XtraFocus pinhole implant. This secondary hydrophobic acrylic sulcus lens has a clear central optic that can reduce dysphotopsia and aberrations caused by iris anomalies. An FDA trial is currently underway. Watch an Eyetube video overview of this implant that includes several interesting cases.
Conclusion
Iris anomalies are rare, but when we encounter symptomatic patients, there are options to alleviate undesired visual effects and enhance appearance. Due to the delicate nature of the iris tissue, surgical repair requires great care and patience, so finding surgeons comfortable managing these cases may take some research.
Click to View

Share
Questions If you have questions, feel free to contact any of our optometric physicians. We’re always happy to help.
ABOUT THE AUTHOR
Brian Arvidson
PCLI—CHEHALIS, WA
Pleasant, easy going and thoughtful, Brian Arvidson maintains a positive outlook with a light sense of humor. Originally from Ellsworth, Maine, Brian grew up in Pendleton, Oregon. He enjoys spending time with his family, mountain and road biking, as well as playing soccer and serving on eye care missions. Brian and his wife Ashley, a teacher, make their home in Olympia, Washington. They have two sons—Austin and Elliott.
